Division of Coronary Diseases
To medicalstaff



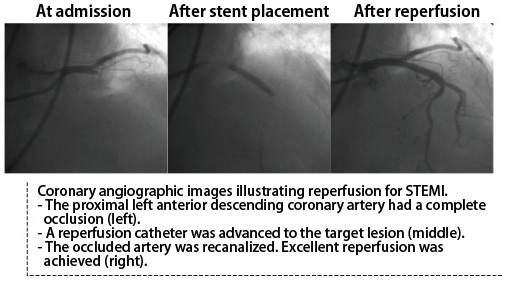 On the other hand, acute coronary syndrome is a serious condition, and starting treatment minutes after symptom onset is critical. ST-elevation myocardial infarction (STEMI), in particular, requires rapid diagnosis and treatment to optimize the clinical outcome.
On the other hand, acute coronary syndrome is a serious condition, and starting treatment minutes after symptom onset is critical. ST-elevation myocardial infarction (STEMI), in particular, requires rapid diagnosis and treatment to optimize the clinical outcome.
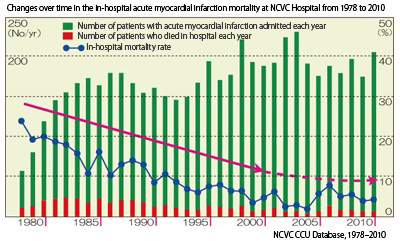
STEMI typically develops when an occlusive thrombus completely blocks an atherosclerotic coronary artery. Thirty or more years ago, the in-hospital STEMI mortality rate at NCVC Hospital was over 25%. Thanks to early catheter reperfusion therapy, clinical outcomes at NCVC Hospital have improved dramatically, with in-hospital mortality rates falling below 5% (see Figure below). Treatment outcomes of patients with STEMI depend on the timing of the intervention relative to symptom onset. Many patients who start catheter reperfusion within 1 hour of onset have complete long-term recovery in electrocardiographic and cardiac function, with no elevations in creatine kinase (CK) or other muscle enzymes.
 On the other hand, patients who arrive at the emergency department several hours after symptom onset often fail to achieve complete recovery of cardiac function. They may experience recurrent episodes of heart failure after discharge.
On the other hand, patients who arrive at the emergency department several hours after symptom onset often fail to achieve complete recovery of cardiac function. They may experience recurrent episodes of heart failure after discharge.
Coronary Computed Tomography (CT) Angiography
Coronary arteries are blood vessels that deliver blood supply to the heart muscle. Angina pectoris develops when the blood supply is impeded by atherosclerotic coronary stenosis. Conventionally, we recommended cardiac catheterization tests for patients with suspected angina pectoris. However, they sometimes refused the test out of fear or anxiety. The advent of coronary CT angiography is good news for such patients.
 More Than 1,500 Persons Undergo Coronary CT Angiography Each Year at NCVC Hospital
More Than 1,500 Persons Undergo Coronary CT Angiography Each Year at NCVC Hospital
Coronary CT angiography is usually conducted in an outpatient setting. After entering the scanning room, the patient will spend about 20 minutes getting an intravenous infusion of an iodine-containing contrast medium with monitoring of their pulse and other vital signs. The CT scan itself lasts approximately 5 minutes.
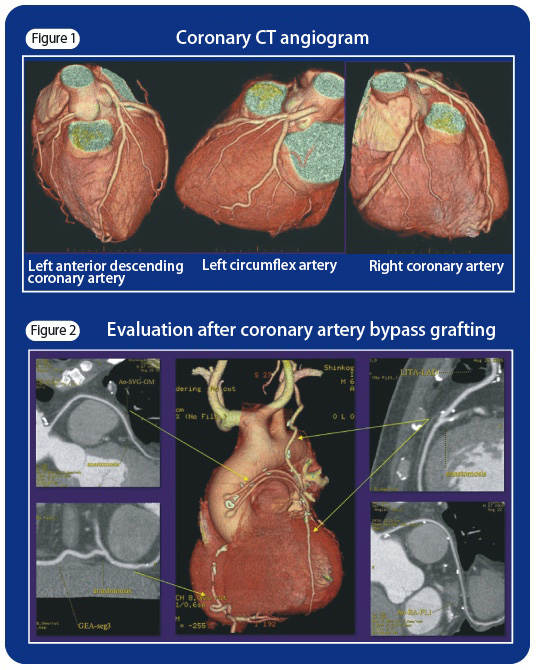
Figure 1 shows three-dimensional surface renderings of the heart and coronary arteries on a CT angiogram. Coronary CT angiography enables assessment of the severity of stenosis (narrowing) of native and grafted coronary vessels (Figure 2). Coronary CT angiography also enables assessment of the severity of atherosclerosis. This information is valuable because arteries with mild stenosis sometimes have advanced atherosclerosis.
NCVC Hospital has installed one of the latest CT scanners on the market. We perform more than 1,500 coronary angiography procedures every year.
Since the end of 2011, NCVC Hospital has adopted a new booking system for outpatient coronary CT examinations. Under this system, NCVC-affiliated primary care physicians can make reservations for their patients.
If you suspect that you have angina pectoris or are concerned that diabetes mellitus increases your risk of angina pectoris and myocardial infarction, please feel free to contact us through your primary care physician.
last updated : 2021/10/01